Betadine oral rinses for covid and other viral infections
2Gordon Seidoh Worley
2Elizabeth
1Ebenezer Dukakis
New Comment
I'm somewhat confused. I may not be reading the charts you included right, but it sort of looks to me like just rinsing with saline is useful, and that seems like it should be extremely safe and low risk and just about as effective as anything else. Thoughts?
Another possible risk: Accidentally swallowing the iodine. This happened to me. I was using a squeezable nasal irrigation device, I squirted some of the mixture into my mouth, and it went right down my throat. I called Poison Control, followed their instructions (IIRC they told me to consume a lot of starchy food, I think maybe I took some activated charcoal too), and ended up being fine.
Before we get started, this is your quarterly reminder that I have no medical credentials and my highest academic credential is a BA in a different part of biology (with a double major in computer science). In a world with a functional medical system no one would listen to me.
Tl;dr povidone iodine probably reduces viral load when used in the mouth or nose, with corresponding decreases in symptoms and infectivity. The effect size could be as high as 90% for prophylactic use (and as low as 0% when used in late illness), but is probably much smaller. There is a long tail of side-effects. No study I read reported side effects at clinically significant levels, but I don’t think they looked hard enough. There are other gargle formulas that may have similar benefits without the risk of side effects, which are in my queue to research.
Benefits
Math
One paper found a 90% decrease in salivary viral load after mouthwash use (which probably overestimates the effect). Another found a 90% reduction in bad outcomes, with treatment (in mouth, nose, and eyes) starting soon after diagnosis. I suspect both of these are overestimates but 1. 90% reduction is a fantastic upper bound to have 2. Neither of these looked at prophylactic use. A third study found a significant reduction in viral DNA after usage, but did not quantify that by viral load or outcomes.
I feel like if povidone iodine was actually that good we’d have heard about it before. OTOH mouthwash formulations are barely available in the US, and most of these studies were in Asia, so maybe it went to fixation there years ago and the west is just catching up.
So I’m going to call this 9-45% reduction in illness timeXintensity when used after symptom onset. Before onset ought to be higher, my wild ass guess is up to 90%.
One reason I think earlier use is better is that, at least with covid, most of the real damage happens when the virus reaches the lungs. If iodine gargles can form a firewall that prevents an upper respiratory infection from becoming a lower respiratory infection, you’ve prevented most (although not all) of the worst outcomes.
Papers
I livetweeted every paper I read, collected here. I don’t want to brag, but those tweets were very popular among ladies with large boobs and 10 numbers in their twitter handles. So if that’s your type you should definitely check out those threads. Everyone else will probably find them tedious, so I’m going to summarize the most relevant papers here.
Estimating salivary carriage of severe acute respiratory syndrome coronavirus 2 in nonsymptomatic people and efficacy of mouthrinse in reducing viral load: A randomized controlled trial
This study had participants rinse their mouth with one of four mouthwashes, and compared the pre-mouthwash salivary viral load with the viral load 15 and 45 minutes later. The overall effect was very strong: 3 of the washes had a 90% total reduction, and the loser of the bunch still had a 70% reduction (error bars fairly large).
Note that despite the title, they only gave mouthwashes to participants with symptoms.
My guess is this is an overestimate of impact, because I expect an oral rinse to have a larger effect on saliva than on cellular levels. I wish they’d tested 4-6 hours later, after the virus had had some time to regrow.
Effect of 1% Povidone Iodine Mouthwash/Gargle, Nasal and Eye Drop in COVID-19 patient
On one hand, this paper features significant ESL issues, missing data, terrible presentation of other data, and was published in a no-name journal. On the other hand, it had one of the best study designs and 30x the number of participants of other studies. I’d love to discard this paper but there aren’t better options.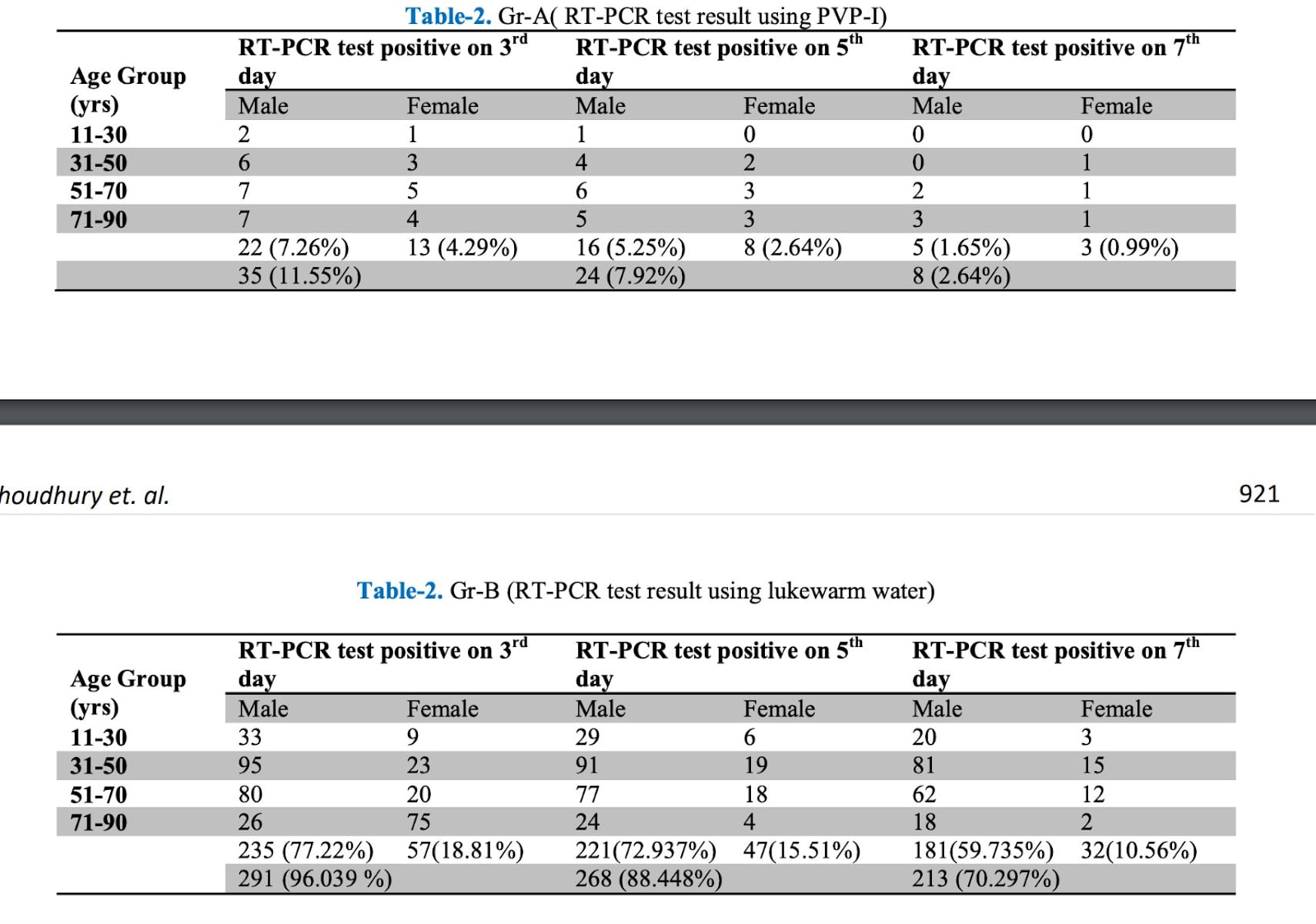
We see an almost 90% reduction in testing positive on the third day. I suspect that overstates the results because it lowers salivary or nasal fluid viral load more than cellular load, so let’s look at outcomes:
90% reduction in hospitalization, 85% reduction in oxygen use, and 88% reduction in death.
I was skeptical of these numbers at first, especially because they only tell you the total number of an age/sex group in the study, and the number of people in a demographic group with a bad outcome. Their percentages also don’t work out properly, making it hard to see the real impact.
Luckily almost everyone in the control group was still PCR positive on day 3, which is almost like having a participant count. The number of control participants still sick on day 3 is indeed about half of every demographic. This doesn’t rule out trickier stuff like putting people at the higher end of their age band in the control group, but it’s a good deal better than that one paper where the youngest person in the control group was a year younger than the oldest person in the treatment group.
The short-term effect of different chlorhexidine forms versus povidone iodine mouth rinse in minimizing the oral SARS-CoV-2 viral load: An open label randomized controlled clinical trial study
I originally ignored this paper, because it only reported Ct values and not outcomes or viral load.* However the previous two papers are from the same author and have shockingly concordant results, and I wanted a second opinion.
[*Ct value = how often you have to run the PCR machine on a sample to get over a particular threshold. This corresponds to viral load but the relationship is complicated and variable. A higher Ct value means lower viral load]
The most important finding is that Ct went up by 3.3 (S genes) and 4.4 (E genes).
N=12 so I’m not thrilled with this study, but pickings are slim.
Side Effects, Or: Should I just gargle iodine all the time then?
Barring very specific circumstances, I wouldn’t. There are several issues that give me pause about long term continuous use.
Hyperthyroidism
Povidone iodine skin washes can cause hyperthyroidism in infants. Among adults, many studies found increases in Thyroid Stimulating Hormone (an indicator of issues but not itself terrible), but not T3 or T4 (directly casual to outcomes). These studies tend to be small and in some cases used the wrong statistical test that missed a long tail clearly visible in their plots, so I assume there exist people for whom this creates a clinically significant effect, especially after prolonged use.
I didn’t include this paper when calculating health benefits, because its control group was too different from its treatment group. But it’s still potentially useful for tracking side effects (although at n=12, it’s still pretty limited). It found a 50% increase in TSH after a week of treatment, but no change in T3 or T4. TSH returned to normal within 12 days of ceasing treatment. That’s not worrisome for healthy people on its own, but could easily reach worrisome with longer use or a vulnerable patient.
Tissue damage could leave you worse off?
There is a long history of aggressive use of topical antimicrobial treatments leaving users worse off due to long term tissue irritation. This is why proper wound treatment changes every decade. That same study looked at this and found no increase in cellular irritation in the throat after six months of use. It’s possible they didn’t look hard enough, or they didn’t have sufficient sample size to catch the effect. It’s also possible the species that invented ghost peppers for fun has a throat surface built to handle irritation and iodine is too weak to hurt us
Oral microbiome damage could leave you worse off?
No one studied this at all, but it looks to me like an obvious failure point. I already use oral probiotics, but if I didn’t I would add them in while using iodine.
How to use
0.5% povidone iodine is sold under the brand name Betadine. You can also buy more concentrated povidone iodine and dilute it yourself. You might be tempted to use a higher concentration, but: 1. Remember the long tail of side-effects. 2. There’s some weird evidence that higher concentrations are less effective. I didn’t dig into this very weird claim but you probably should if you plan to try it.
The Betadine bottle recommends gargling 10ml for 30s, 4x/day. The short term studies used 4-6x/day. Spacing that out is nontrivial attention tax, so when I was sick I just put the bottle on my bathroom sink and used it every time I used the bathroom. This probably comes out to more than 6x/day (especially when I’m sick and chugging fluids), but I also didn’t use a full 10ml and rarely made it to a full 30s, so hopefully it balanced out.
More Data Needed
The state of existing knowledge around iodine gargles is poor. This is especially frustrating because I don’t think it should be that challenging to gather more. I’m toying with a plan to fix this, but will publish separately since it’s not specific to iodine.
For financial support I would like to thank my Patreon supports and Lightspeed grants.